Abavubuka mwenyigire mu bulimi - Kabaka awadde amagezi:
8th December, 2014
By Dickson Kulumba ne Paddy Bukenya
Kabaka ng’awuubira ku bantu be ku mbuga y’eggombolola y’e Buwama mu ssaza ly’e Mawokota e Mpigi ku Lwomukaaga ku mikolo gy’Abavubuka mu Buganda.
KABAKA Ronald Muwenda Mutebi II alagidde abavubuka okwongera okwegatta
beenyigire mu bulimi nga balima ebirime eby’ettunzi okusobola okwekulaakulanya.
Omutanda ng’ali ku mikolo gy’abavubuka mu Buganda ku mbuga y’eggombolola y’e Buwama mu ssaza lya Mawokota mu disitulikiti y’e Mpigi ku Lwomukaaga, yawadde abavubuka amagezi okukozesa ebifo ku masaza ne ku magombolola okukolerako emirimu egy’enjawulo egy’enkulaakulana
n’asiima abatandiseewo emirimu ne bayambako n’abalala okwebeezaawo.
Ente Omubaka Kenneth Kiyingi Bbosa (Mawokota South) gye yatonedde
“Omwaka guno tujjukiziddwa ensonga y’ebyobulamu. Abavubuka tusaanye okwekuuma nga tuli balamu, okwekebeza buli mwaka kubanga si kirungi okugenda mu ddwaaliro nga tumaze okugonda ate omuvubuka alina okulya obulungi.”
Katikkiro Charles Peter Mayiga yakunze abavubuka okukozesa emikisa Kabaka gy’abatee
reddewo; mu by’obulimi beekwate BUCADEF n’okuyingira Ssuubiryo Zambogo SACCO.
Omulamwa gwabadde; Omuvubuka omulamu ate nga mukozi ye nnamuziga w’enku
laakulana mu Buganda, era wano Minisita w’abavubuka e Mmengo, Henry Ssekabembe, we yategeerezza nga bammemba ba Ssuubiryo Zambogo SACCO bwe batuuse ku 1,500 nga kati balinawo n’obukadde 285.
Abamu ku Baamasaza ku mukolo gw’Abavubuka mu Buganda e Mawokota ku Lwomukaaga.
Omukolo gwetabyeko; ssentebe w’abavubuka mu Buganda, Richard Kabanda, Kayima David Ssekyeru, Katikkiro eyawummula Dan Mulika, sipiika wa Buganda Nelson Kawalya n’omumyuka we Ahmed Lwasa, Minisita Amelia Kyambadde, Omubaka Kenneth Kiyingi Bbosa (Mawokota South) ssaako baminisita b’e Mmengo, abakulu b’ebika n’Abaamasaza.
Abayimbi; Mathias Walukagga ne Fred Ssebbale be baasanyusiza abantu ba Kabaka.
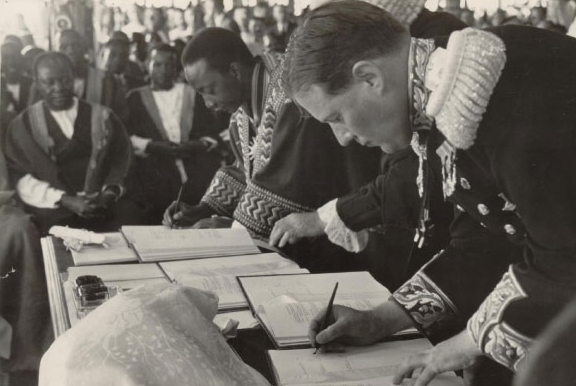
The first bank in The Ganda Kingdom:
By Henry Lubega
Posted Sunday,1 st March, 2015
Before 1906, there was no banking institution in Uganda until November of the same year when the national Bank of India opened its first branch in Entebbe, and four years later it opened the first bank in Kampala, although it was later taken up to become Grindlys Bank.
The National Bank of India was followed by Standard Bank of South Africa Limited when on September 19, 1912, it opened its first branch in Kampala. And a few years later it opened another branch in Jinja.
Barclays
Barclays followed in 1927 when it opened two branches in Kampala and Jinja. In 1954 three more banks; Bank of Baroda, Bank of India and The Nedelandsche Handel-Maatschappij M.V (Netherlands Trading Society) opened in Uganda.
According to Saben’s commercial directory and handbook of Uganda, as early as 1949 the banking system had been established in Uganda but did not control much of the financial liquidity that was in circulation across the board in the country.
“Much of the money was controlled in the bazaars and other channels which were predominantly controlled by people of the Asian origin. These people played a key role in the buying of cotton.
However, areas where banks were non-existent, merchants in those areas played the part of the banks. This was through taking drafts in exchange for cash or physical items in exchange for hard cash,” Saben wrote.
By 1950, it was realised that to bring more Africans into the business there was need to provide them with credit. Unfortunately, the commercial banks at the time would not extend credit to Africans because of the nature of their securities.
Under Ordinance number 20 of 1950 the Uganda Credit and Saving Bank was created purposely to extend credit facilities to Africans with the aim of furthering agriculture, commercial building and co-operative society purposes.
On October 2, 1950, the bank was opened and by 1961 it had spread to places like Arua, Fort Portal, Jinja, Soroti, Gulu, Masaka and Mbale, taking only African deposits.
Building Society
Two years later, the first Building Society in Uganda was opened as a subsidiary of a Kenyan owned firm Savings and Loans Society Limited.
More financial institutions continued to open up in Uganda with Lombard Bank from Kenya, in partnership with Uganda Development Corporation, opening the Lombank Uganda Limited in 1958. It was this bank which first introduced the hire purchase system of shopping in Uganda.
It was not until 1966 that through an act of Parliament that Bank of Uganda was created. Prior to this, issues to do with money were handled by the East African currency board which had its head offices in Kenya.
African Traditional Revenue and Taxation:
Money in dollar bills seized from a home of the Commissioner General of the Tanzania Revenue Authority is pictured down: Over 20 bags of it:
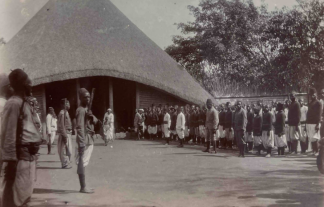
OBULANGO
Oluguudo Lwa Kabaka Njagala, Mubweenyi
bw'enju ya Kisingiri ewa Musolooza.
Telephone::
Ssentebe - 256 712845736 Kla
Muwanika -256
712 810415 Kla
UGANDA.
Email Links:
info.bazzukulu
babuganda
@gmail.
com.
OMUZIRO:
NKEREBWE
AKABBIRO
Kikirikisi-Mmese etera okuzimba mu kitooke.
OMUTAKA
KIDIMBO.
OBUTAKA
BUDIMBO.
ESSAZA
SSINGO
OMUBALA:
Nkerebwe nkulu esima nga eggalira
Olukiiko lwa Buganda lwanjudde embalirira ya buwumbi 7
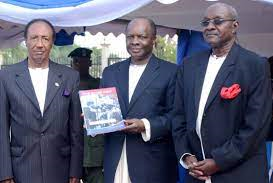
The Kabaka of Buganda launches a book on Ssekabaka Muteesa II struggles:
Posted Friday, 27 May, 2016
By the Monitor, Uganda
Kabaka Mutebi (centre) with Mr Patrick Makumbi (right) and Dr Colin Sentongo (left) at the book launch at Bulange in Mengo, Kampala.
Kampala in the State Kingdom of Buganda:
Kabaka Ronald Mutebi on Wednesday, 25th May 2016, launched a book about the struggles of his late father and former Buganda king, Edward Muteesa II, touching on Uganda’s history before and after independence.
The book titled The Brave King, revisits the stories of Muteesa’s exiling, first between 1953 and 1955, and again from 1966 to 1969 when he died in London. The author, Mr Patrick Makumbi, drew from the documents preserved by his father, 99-year-old Thomas Makumbi, who was an official at Mengo, Buganda’s power capital.
“I was very happy to write the preface to this book,” Kabaka Mutebi said, adding: “It will help the readers understand what Kabaka Muteesa went through in those days.”
When Mutesa was exiled in 1953, the older Makumbi, the father of the author, led a team of six Buganda officials to negotiate with the British about the king’s return to Buganda, which was secured in 1955. The other members of the team were Mr Apollo Kironde, Mr Matayo Mugwanya, Mr Amos Sempa, Mr Eridadi Mulira and Mr Ernest Kalibbala.
Kabaka Mutebi, while officiating at the function, called on more people to document what they saw during those days, saying “it is a good thing” that some of those who witnessed or participated in the events are still alive. Muteesa himself wrote about the period in question in his autobiography, The Desecration of my Kingdom, and Kabaka Mutebi’s endorsement of Mr Makumbi’s new book will be seen as an extension of the kingdom’s bid to manage the narrative.
Mr Apollo Makubuya, Buganda’s third deputy Katikkiro, at the launch held at Bulange-Mengo said there have been attempts to misrepresent history by “those who do not like us”.
Accusations and counter accusations of betrayal between Buganda Kingdom and Obote are rooted in a rather happy start, when Buganda’s party Kabaka Yekka (KY) teamed up with Obote’s Uganda People’s Congress to defeat the Democratic Party and form government at independence in 1962.
But the two centres of power soon quarrelled violently and were involved in what many have regarded as a critical turning point in Uganda’s history. The army, on Obote’s orders, stormed Muteesa’s palace on May 24, 1966, killing multitudes and forcing the king-president into exile.
Mr Makubuya said his grandfather was among those killed during the attack, an occasion the kingdom commemorates yearly on May 24. He said in addition to explaining how Buganda and Muteesa suffered during that period, Mr Makumbi’s book will clarify a number of other issues, including how colonialism thwarted Buganda’s development efforts.
He said Buganda stiffly resisted colonialism and the demands of colonial governor Andrew Cohen in particular, to the extent of winning a court case in London against the exiling of Muteesa. In all its efforts, Mr Makubuya said, Buganda was consistently seeking autonomy, and that the kingdom can “never” lose sight of this objective.
Mr Makumbi, the author, said his father could not attend the launch due to old age.
The publication of the book was financed by Dr Colin Sentongo, who said at the launch that KY, which ceased to exist in the 1960s, is the only political party he has ever belonged to.
The fathers of Mr Makumbi and Dr Sentongo met with Muteesa as students at Kings College Budo, from where, Mr Sentongo said, the three men forged a life-long friendship. It is probably much for this reason that Kabaka Mutebi warmed up to Mr Sentongo and Mr Makumbi at the launch.
emukiibi@ug.
nationmedia.com
Fiscal Budget y'Ensi Buganda ebiro bino:
Posted 7th July, 2014
By Dickson Kulumba
Omuwanika wa Buganda, Eve Nagawa Mukasa
Omukyala Eve asomye embalirira y’Obwakabaka bwa Buganda eya 2014/2015 nga ya buwumbi 7 (7,411,638,600/-) .
Embalirira eno eri wansi w’omulamwa 'Okwolesebwa n’Ebigendererwa' egendereddwamu okutumbula enkulaakulana okuli; okumaliriza Amasiro g’e Kasubi ne Wamala, Masengere, okulongoosa Ennyanja ya Kabaka, okussawo etterekero ly’ebyedda, okukulaakulanya ettaka ly’e Kigo ne Makindye 'State Lodge', okuzimba olubiri lw’omulangira Juma Katebe, okuzimba olubiri lwa Namasole, okuddaabiriza embuga z’Amasaza wamu n’okuzimba eddwaliro ly’abakyala.
Nagawa yagambye nti ensimbi zino zisuubirwa okuva mu Buganda Land Board, Amasomero, Minisitule ez’enjawulo, mu bupangisa, amakampuni g’Obwakabaka, ebitongole ebigaba obuyambi n’obuwumbi buna okuva mu Gavumenti eya wakati.
Ng’ayogera mu lukiiko luno, Katikkiro Charles Peter Mayiga yasabye abantu okutambulira ku kiragiro kya Kabaka eky’abantu okujjumbiro ebifo by’obulambuzi era n'ategeza nti pulojekiti zonna Obwakabaka ze butandiseeko ssi zaakukoma mu kkubo, zirina okumalirizibwa n’olwekyo enkola y’okunoonya Ettoffaali ekyagenda mu maaso kubanga Kabaka ayitibwa mufumbya Gganda n'antabalirira batyabi- ensimbi zikyetaagisa.
Olukiiko luno lwetabiddwamu abakiise bangi ddala ne baminisita ba Kabaka nga lwakubiriziddwa, Sipiika Nelson Kawalya eyagambye nti embalirira eno abakiise basaanye okugenda n’ekiwandiiko kino, bwe banakomawo mu lukiiko luno basobole okugiyisa.
Jinja regional referral Hospital has had its management questioned over what is now referred to as the biggest mistake in Uganda’s medical history.
The graphic image, Baby whose limp was cut by an intern doctor
This is after a mother had his newborn’s arm chopped off during a Caesarean delivery by a doctor who authorities have learned was an intern at the medical facility.
Are you on Instagram? Click the button below, follow us for daily exclusive news and videos
A source, also a doctor at the facility told authorities that the mother came to the hospital for checkups after her pregnancy started showing complications but was later discharged by one Dr. Thomas Data who is also an intern.
A graphic photo of detached arm taken at the hospital
The mother returned to the hospital bleeding and according to our source, asked for a particular doctor, Dr. Mathias Ngobi who had handled her with care to take care of her and help her deliver.
Little known to the mother, Dr. Ngobi was also an intern at the facility. Doctor Ngobi assessed the bleeding mother and concluded she was bleeding from an intrauterine fetal death and quickly suggested a C-section to remove the dead fetus.
NBS Uganda news headlines
Dr. Ngobi assisted by Lovensa Nakabito took to the lady into theatre and began their C-section. Upon cutting open of the abdomen, a previous C section wound burst open, too much blood started coming out making it difficult for the intern doctor and his assistant to navigate.
Known to them that the baby inside was dead, they forced the baby out with their equipment detaching an arm from the baby. Shock dawned on them when they found out that the baby was alive.
The baby’s father has since disappeared after taking pictures of his baby with a butchered arm. Authorities want the hospital management to come out with a conclusive report of how the incident happened before they could take action.
The Parliament of Uganda has asked the government of Uganda to upgrade the dilapidated morgues all over the country:
By Moses Walubiri, Moses Mulondo
Added 8th May 2019
A number of reports by Auditor General have over the years highlighted a breakdown of refrigeration services in government hospitals.
The Kampala city mortuary is one of such facilities in need of a makeover. File Photo
Jacob Oulanyah, the Deputy Speaker of Parliament has asked the Ministry of Health to fix rundown mortuaries after a section of lawmakers reported dysfunctional morgues in a number of regional referral hospitals.
Oulanyah’s complaint followed a complaint by Lyandro Komakech (Gulu Municipality) that an investigative journalist working with a local TV station exposed two badly decomposing bodies at Gulu Referral Hospital.
“The footage was so disturbing and we demand that the director of the hospital be relieved of his duties,” Komakech said.
Joseph Gonzanga Ssewungu (Kalungu West) told the House that the situation in Gulu is a microcosm of the dire situation concerning dysfunctional morgues in different parts of the country.
“For us in the greater Masaka, dead bodies are left in wards because mortuaries are dysfunctional. This has taught many people to stop fearing dead bodies,” Ssewungu said, adding: “Let the ministry of health produce a status report on all mortuaries in the country.”
The mortuary at Mulago Hospital. File Photo
Minister of state for health, Dr Joyce Moriku Kaducu pushed back against calls to have the director Gulu Referral Hospital sacked without giving him a hearing.
“The bodies in issue were dumped by unknown people and it’s the duty of Gulu municipality to bury unclaimed bodies in its locality, not the hospital,” Kaducu said.
However, instead of tabling a status report on morgues in the country, Oulanyah asked the health ministry to fix all mortuaries to avert the dangers that come with failure to properly preserve dead bodies.
A number of reports by Auditor General, John Muwanga have over the years highlighted a breakdown of refrigeration services in government hospitals.
Where the refrigeration services are working, some of the public health facilities have intermittent power supply which results in poor preservation of cadavers.
My six-year battle with prostate cancer in the expensive national hospitals of Uganda:
Although there are usually no symptoms during the early stages of prostate cancer, it is important to teach yourself and know what to look out for. This is the reason Otim is still alive today. COURTSEY PHOTO
19 November, 2018
By Joan Salmon
“I would frequent the toilet to urinate, sometimes more than four times in one night,” says Willie Otim, 71. The father of six, retired from civil service in October 2010 and up to that time, he had never battled with disease and was physically fit and healthy. However, towards the end of 2012, he started experiencing problems with his urinal system.
Otim says even after urinating, he still felt that he needed to urinate despite no urine coming forth. At first, he thought it was a urinary tract infection and immediately started visiting a number of clinics in Lira Town for treatment. Unfortunately, none of them was able to diagnose the disease as cancer and because he was living with diabetes, Otim pegged the frequent urination to the disease.
Diagnosis However, despite religiously taking his diabetes medication, the situation did not change at all. In fact, his health deteriorated until he decided to travel to Kampala for treatment. He first visited International Hospital Kampala (IHK) and specifically told them he wanted to see the hospital urologist.
“I was referred to Dr Frank Asiimwe, a urologist. He examined me thoroughly and suspected that I could be having prostate cancer but needed confirmation by carrying out other tests. One of the tests was checking for Prostate-specific antigen (PSA), a substance produced by the prostate gland,” he says. Elevated PSA levels may indicate prostate cancer, a noncancerous condition such as prostatitis, or an enlarged prostate.
Otim adds that since he also needed to undergo a magnetic resonance imaging (MRI) scan, he was referred to Mengo MRI Centre while PSA level was checked at IHK.
“My PSA level was found to be at 11.8 which is way above the normal level of a person free from prostate cancer. The MRI scan also confirmed that I had prostate cancer,” Otim reveals. It was then recommended that he goes for an operation to remove the cancer. A normal PSA level is considered to be 4.0 nanograms per milliliter (ng/mL) of blood. For men in their 50s or younger, a PSA level should be below 2.5 in most cases. Older men often have slightly higher PSA levels than younger men.
The operation The operation was done on February 8, 2013 at Mulago National Referral Hospital. “At the time, the hospital lacked one very important equipment in the theatre without which my operation would not be possible. The equipment was hired at Shs650,000, which I had to pay,” he narrates. Thankfully, the operation was successful. However after, blood and urine continued to ooze from the operated area which called for another operation. After a few days, he was discharged but still experienced a lot of pain and had to use a catheter for urinating. The catheter was later removed because it was associated with frequent infections. The uncontrollable pain continued for some time until a scan was requested. “The scan showed that some gauze had been left in my stomach after the operation. Thankfully, it was successfully removed after which I felt very comfortable,” he says.
Treatment He was then referred for radiotherapy with the aim of killing any cancerous cells that might have remained after the operation. “In 2013, Mulago National Referral Hospital had an old radiotherapy machine serving many cancer patients that we had to arrive at the treatment room as early as 5am. I was given five dozes of radiotherapy,” Otim says. While undergoing radiotherapy, Otim says he felt extremely weak, passed blood stained stool and lost appetite. To counter some of these side effects, he was advised to take a lot of fluids, some of which were expensive. “Taking fresh fruit juice on a daily basis can indeed dig deep into one’s pocket,” he adds.
Review After radiotherapy, Otim was advised to go for review after every three months. He did that all through 2015 and 2016, after which he stopped because he thought he was cured. “This was a mistake on my part because the review was supposed to be continuous and indeed, in late 2017, I started feeling back pain and getting restless,” Otim regrets.
He once again visited a few clinics where he was treated but there was no relief. After a short while, he had a bad experience where the nerve around the pelvic region started sending some kind of electric shock waves from his waist region to the feet. The following morning, he awoke only to find his legs paralysed.
“I was unable to balance my body, let alone walk. I then decided to travel back to Kampala for better diagnosis,” he says. In Kampala, he went to IHK where he was admitted right away. “They took long to diagnose the problem and after one week, I was sent for another MRI scan at Mengo hospital where it was discovered that the cancer had affected my spinal cord, hence the paralysis,” he shares.
I was referred to Mulago Cancer Institute. “I spent six days at IHK and it cost me Shs6.5m in hospital bills,” Otim says. Admission to Mulago Cancer Institute would see him spend two weeks there and paying Shs100,000 everyday. This time, he received six doses of chemotherapy, of which each was administered after every 21 days. The effects of the chemotherapy were not any different from those of radiotherapy as he still felt extremely weak, passed blood stained stool, lost appetite and hair.
The review period was also after every three months and he was also advised to go for physiotherapy which he has been doing for the last one month. “I must say the physiotherapy has helped as I have been able to abandon the wheelchair and the four legged walker,” he says with a smile. He now comfortably uses crutches and has also been praying to the Lord for total recovery.
Screening This November, UMC Victoria Hospital is encouraging men to “man up” and take action to live healthier, happier and longer lives by screening for prostate cancer.
Screening is available at all the UMC Hospitals in Bukoto, Kira road, Nakawa and Entebbe freely this November but can go for a fee of Shs80,000 after November.
Challenges • Diagnosis of prostate cancer is very expensive. Willie Otim says to carry out an MRI scan he had to pay Shs750,000 while the second time, it cost him Shs1.5m. • He also says facilities such as laboratories dedicated to testing for prostate cancer are not readily available in district hospitals except at Mulago National Referral Hospital. He had to travel from Lira every time he needed treatment. “The journey is so laborious, especially when you are not feeling well,” he says. • He adds that cancer drugs are not always available at Mulago national Referral’s pharmacy which left him with only one option of buying the medicine from private pharmacies whose prices are so high. • There is an ever increasing number of cancer patients yet the facilities are not increasing in number. For example, there were times when he and other patients would have to be placed in the corridor due to lack of space. • The number of doctors specialising in cancer treatment is small. That means that the lines to see the few doctors available are long. He was restricted to a wheel chair and that greatly inhibited his movements and increased his dependency on people.
jsalmon@ug.nationmedia.com
In Uganda, a Mother has stabbed a medical staff to death at Soroti hospital:
Soroti Regional Referral Hospital is situated 320Km North –East of Kampala. It became a district hospital in 1978 and was elevated to a regional referral status in 1996. It is the main government referral facility for the mid-eastern region of Uganda with a bed capacity of 274.
November 12, 2018
Written by URN
A 20-year-old mother has stabbed her attendant to death. The two had reportedly disagreed on a ploy to escape from Soroti regional referral hospital where, the woman, identified as Paska Angela had a caesarian birth last evening.
The deceased, a resident of Oyomai village, in Kaberamaido district, is a mother-in-law to Angella, a resident of Koidike village-Iriiri parish, in Napak district. According to eyewitnesses, the suspect wanted to escape with her relatives but was blocked by her mother-in-law. It is not immediately clear why the suspect wanted to escape and how she obtained the knife that she reportedly used to stab her mother-in-law.
Esther Akol, one of the eyewitnesses narrated that the suspect lured the caretaker, a mother of eight to the bathroom at around 2:00am and stabbed her in the chest. Dr Ekunait Oumo, one of the senior doctors at Soroti hospital said the deceased was hit on the low pressure point leading to her immediate death.
Angella was arrested as she tried to escape from the facility early today. She is now detained at Soroti Central Police Station.
Angry relatives of the deceased that had camped at the hospital attempted to grab Angella from the police that was taking her for medical examination, saying she equally deserved to die.
East Kyoga region police spokesperson Michael Odongo said that the doctor had advised them to take the suspect for further medical examination but they were forced to flee the premises when the angry relatives descended on the police.
"We wanted to protect her from the mob that wanted to lynch her," Odongo said.
Nb
It is normal practice in Uganda to confine and arrest patients on hospital beds until they pay for the services they have received.
How the Medical insurance is trying to increase the use of family planning services in Uganda:
By Lillian Namusoke Magezi
Added 19th October 2018
The conclusion was reached after a study conducted in Kalerwe and Kifumbira (both Kampala slums) by GHE (Global Health Economics) Consulting, a health research firm.
PIC: Barriers to family planning include long distances to facilities, the cost, lack of knowledge and the high stigma associated with access to family planning services by the youth
HEALTH
Having medical insurance and using a benefits card to access services has been proven as a way of increasing the uptake of family planning services by the youth in low-income urban areas (slums).
The conclusion was reached after a study conducted in Kalerwe and Kifumbira (both Kampala slums) by GHE(Global Health Economics)Consulting, a health research firm.
The study set out to investigate whether using benefits cards was an incentive to increasing access to comprehensive family planning services for the youth in urban areas.
Janet Babigumira, a research consultant at GHE Consulting, discloses that under the study project, the firm was awarded funding through Grand ChallengesCanada’s Stars inGlobal Health program in 2016.
The funding was meant to support the development of an incentive-based programme to increase uptakeand reduceunmet need for modern family planningmethods among the youth (18 - 30 years) living inlow-income urban areas like slums in Kampala district.
She noted that their focus was on family planning for the youth because family planning is a key sectorin promoting the economic growth of the country and it is critical in the achievement of the sustainable development goals.
She added that family planning uptake among the youth is very important because Uganda has a very young population with 50% of the people under15 years and 75% under 25 years.
Minister Kaducu and Commissioner Nsungwa checking on a mother in Kamwenge. Teenage pregnancy is said to decrease according to education level
In addition, the country has a high teenage pregnancy rate at 25%. Therefore, there is need for sustained access to family planning services so as to reduce fertility.
Challenges faced include the fact that the unmet need for contraception are still very high and jeopardize the rights of girls and women to have a safe, healthy and productive life.
She noted that the fast growing population, the high rate of unwanted and teenage pregnancies, in addition to limited access to services are clear evidence that concerted efforts and substantial investments are urgently needed to meet the needs and growing demand for user-friendly and youth-friendly services.
Causes of limited access to family planning
Elly Nuwamanya, a research analyst at GHE Consulting, noted that they set out to pilot the project after evidence showed that young people face barriers in accessing family planning tools and services.
Information from the health ministry shows that such barriers include long distancesto facilities, the cost, lack of knowledge and the high stigma associated with access to family planning services by the youth.
Other issuesare unfriendlinessof the health workers, limited variety of family planning methods, long waiting hours, stock-out of commodities and fear of side-effects.
Others are partner’s disapproval, religious/ cultural beliefs that discourage people from uptakeand lack of other sexual and reproductive health services such as treatment of STDS at the facility.
As aresult of the above challenges, there is a high unmet need for contraception among the youth in Uganda, which leads tounplanned pregnancies (resulting in unsafe abortions) and sexually-transmitted infections(STIs).
Use of health card
Babigumira explains that the programme was designed based onan insurance model where a premium was charged for every beneficiary.
However, she adds that throughfunding from Grand Challenges Canada, the premium was paid by the project and the recruitedparticipants received the cards for free for a period of six months.
The card allowed thebeneficiaries to access family planning services, HIV/AIDSservices (counseling, testing, guidance, referralsand follow-up treatment) in addition to pregnancytesting and follow-up care.
Nuwamanyaexplained that the effectiveness of the card was assessed using a controlled studywhere somegroup received the card and another group did not receive the card.He said the group that received the card was in Kifumbira,a slum in Kamwokya, a Kampala suburb;and the control group was in Kalerwe, another slum area.
The two areas are assumed to be of similar social demographic statistics.
Nuwamanya disclosed that the recruited participantswere followed up for a period of six months to assessif there wereany changes in contraceptive uptake and unmet need for child spacing.
In addition, the studyalso assessed theacceptability and usability of the card services for the first six months.
Findings of the study showed that the using a health card was highly acceptable with 93% acceptance rate.
The cards were used for injectable contraceptives (39%), contraceptive pills(29%)and implants (17%).The findings tallied with the UDHS (2016) which showed that injectable contraceptives were the most popular means of family planning at 20%.
Among other services provided by thecard were pregnancy tests (61%)and HIV tests (34%).
Contraceptive use said to be higher in marrieds than the single
A health official explains to the youth about moon beads, a method of family planning
Use of card increases contraceptive uptake
Presenting results from the assessment study in Kampala recently,Nuwamanya disclosed that use of a health card was highly effective in increasing contraceptive uptake and reducing the unmet need forchild spacing.
Results show that modern contraceptive use increased from 34% to 50% among the people who were given the card; and declined from 46% to 44% in the control (those not given the card).
In addition, unmet need for child spacing declined significantlyfrom 55% to 40% in those given the card, and from 38% to 37% in the control group.
The study also discovered that the satisfactionindex (a measure of satisfaction with family planning services) increased significantlyfrom 24to 28 among those that had the card, but reduced from 24 to 23 in those who did not have the health card.
Other findings
Nuwamanya noted that the study also showed that:
Overall, contraceptive use was higher among the married (48.3%) than the single (34.6%). Contraceptive uptake is poor among single people and those who have never given birth because of misconceptions and fear of assumed side effects
Awareness of family planning was also positively related with increase in contraceptive use.
Short term methods of family planning were preferred over long-term.This could be due to the fact that the participants in the study were still young and seeking to grow their families.
Fewer men go for HIV testing and counseling.
Teenage pregnancy decreased with education level
No education 42%
Primary 36.5%
Secondary 25.9%
Secondary plus 10.3%
An official from PATH talks to the youth on how to avoid early pregnancies
From the above findings, the research team concluded that having an insurance card was anincentive to attract the youth to access family planning services.
Gaps noted
However beneficiaries noted that in addition to family planning and HIV/AIDS services, the cards also needed to have covered testing and treatment for other sexual and reproductive health conditions such as STDs.
Way forward
Dr. Frank Asiimwe, a clinical research associate at GHE Consulting,noted that as we transition to scaling up the programme, there is a plan to expand it to all urban youths in Kampaladistrict.
This is in addition to extending the programme to cover all sexual and reproductive health services.On the issue of affordability of the services, he noted that there is a need to make the cards subsidized or free.
Nuwamanya also added that there is need continue carrying out sensitization about family planning so as to increase people’s awareness and address misconceptions that limit people’s uptake.
He urged policy makers to allocate adequate resources for sexual and reproductive health and create an enabling environment for service delivery and accessibility
Mu Uganda, Eddwaaliro ly'e Bukomansimbi, Buganda State, lisaliddwaako amasannyalaze:
Babanjibwa obukadde bwa shillings 10 nga emyaka 5 tebasasula masanyalaze:
Eddwaaliro lya Butenga Health Centre IV eryasaliddwaako amasannyalaze. Mu katono ye Muhammad Kateregga, Ssentebe wa disitulikiti y'e Bukomansimbi
By Musasi wa Bukedde, Phiona Nanyomo
Added 21st September 2018
Abatuuze b'e Bukomansimbi bali mu katuubagiro olw'eddwaliro erisinga obunene mu disitulikiti eno okusalibwako amasannyalaze nga libangibwa ensimbi ezikunukiriza mu bukadde 10 erimaze ebbanga lya myaka 5 nga terisasulwa.
Eddwaliro lya Butenga Health Centre IV olukiiko lwa disitulikiti eno lwayisa ekiteso likuzibwe okutuuka ku mutendera gwa 'district hospital' nga muno mwe muweerezebwa abalwadde bonna ababeera balemeredde abasawo mu malwaliro agasokerwako mu disitulikiti eno.
Ssentebe wa disitulikiti y'e Bukomansimbi, Muhamed Katerega agamba nti ab'ekitongole ky'amasannyalaze baazinzeeko eddwaaliro lino ne bakutula waya ezirituusaamu amasannyalaze era kati abasawo, abalwadde n'abajjanjabi mu budde bw'ekiro babeera beemagaza bwemagazza olwokubulwa ekitangala kko n'ebyuma ebikolera ku masannyalaze okujjanjaba abalwadde obutasobola kukola.
Kyokka okunenyezebwa ssentebe Katerega akutadde ku bakulira eddwaliro lino nga agamba nti baalemererwa okutwala obuvunaanyizibwa okusasula ssente zino ate nga bafuna ssente okuva mu gavumenti ez'okuddukanya eddwaliro lino.
Ye kansala w'egombolola y'e Butenga, Isaac Lwanga ategeezezza nti okuva eddwaliro lino okuva lwe lyasalwako amasannyalaze abatuuze basanga okusomoozebwa kw'okutambula eng'endo empanvu okutuuka mu ddwaaliro ekkulu e Masaka kko n'eryaVvilla Maria okufuna obujjanjabi obusaanidde.
Kaweefube w'okwogerako n'akulira eby'obulamu mu Bukomansimbi yagudde butaka oluvannyuma lw'okumukubira amasimu ge gonna agamanyiddwa nga tagakwata.
Kinajjukirwa nti gavumenti ya Korea yawaayo obuwumbi bwa ssente za kuno 4 okutumbula ebyobulamu mu disitulikiti y'e Bukomansimbi era ekizimbe galikwoleka ekissiddwaamu ebyuma ebyomulembe kyatongozeddwa ku ddwaliro lino erya Butenga.
Nb
Bano abakungu ba NRM abakwasibwa ebyobulamu bwaffe North Korea oba South Korea bweyabawa ebikozesebwa ebyomulembe ebyennaku zino mumalwaliro balabika baali balinzi era ensi zino zibaleetere ne byuuma bya masanyalaze aga Solar okuddukirira kunkozesa yamasanyalaze ensamusamu eri abalwadde ba Africa abaavu! Bajjajja baffe wano e Buganda kyebava bagamba batya? Etesiima..........
Ffe ebigambo byatuggwako dda abawi bamagezi. Bwetuwandikiira ku Bukedde nga tudamu kunsonga nga zino azitukwatako kubulamu bwaffe nabantu baffe, Bukedde ebyaffe abigana okubitekako. Mbu tuvuma bakozi ba governmenti. Tukyamula abantu bekalakaase bajjeko governmenti eno. Tetulina kulaba bakulu mu kamwa. Emyaka 33 twogere bilungi byerere byetuyitamu ffe nabantu baffe era tuyige okusiima. Tulekere awo olugambo lwa social media. Computer tuzisuule eri, tukwate enkumbi tugende tulimire enjala yaffe wano mu Africa, kasooli.
The British Uganda Aid Biometric machines installed in President Museveni's hospitals has exposed to him many absentee staff at Naguru hospital:
July 22, 2018
Written by URN
Close to 40 members of staff at the China- Uganda Friendship Hospital, Naguru face sanctions for absenting themselves from work and reporting late for duty. The affected persons, mostly medical workers, have been asked by the hospital management to submit written explanations stating why they missed duty for more than 15 days this month. A letter requiring them to submit explanations was signed and stamped by the hospital director bearing the names of 39 implicated staff.
The hospital gates of the Naguru Hospital where China has invested much of its medical skills in Uganda.
Three of the people reported on duty for only one day, while the person who worked more days is recorded as having reported to work for 10 days between July 1 to 19, 2018. Close to 40 members of staff at the China- Uganda Friendship Hospital, Naguru face sanctions for absenting themselves from work and reporting late for duty. The affected persons, mostly medical workers, have been asked by the hospital management to submit written explanations stating why they missed duty for more than 15 days this month. A letter requiring them to submit explanations was signed and stamped by the hospital director bearing the names of 39 implicated staff. Three of the people reported on duty for only one day, while the person who worked more days is recorded as having reported to work for 10 days between July 1 to 19, 2018.
Nb
One reckons the Uganda African patients have been well aware of what has been going on for some good years. It is unfortunate that the former colonialists of Great Britain with their biometric machine are the one making the African hospital management aware of this hospital administration mismanagement.
Uganda has finally got a decent hospital for its long time suffering patients:
Inside Mulago Hospital’s sh91.5b maternal health centre:
By Violet Nabatanzi
Added 4th July 2018
This will be the first public health facility providing fertility-related services
Mulago National Referral Hospital’s state of the art national maternal and neonatal referral centre that cost $34.14m (about sh91.5b) will open its doors to the public in July.
The centre whose construction began in 2013, will offer specialised treatment for high-risk antenatal care, delivery and postnatal services, gynaecology services, focusing on obstetric fistula.
Mulago Hospital’s Enock Kusaasira touring the new specialised maternal and neonatal center. Photo by Mary Kansiime
Arabs Contractors’ Tarek Eldakdoky (left) giving t Kusaasira a tour of the center. Photo by Mary Kansiime
Speaking to New Vision Mulago’s spokesperson Enock Kusasira said it will also handle cancers of the female reproductive system including ovarian cancer, uterine, endometrial, cervical, and vulvar cancer.
Other services to be offered include neonatal services and In Vitro Fertilisation (IVF). The IVF is a process that increases the efficiency of human reproduction, which is often not efficient naturally.
This will be the first public health facility providing fertility-related services. In Uganda, fertility services are expensive; one has to pay between sh10m and sh20m to access such services in private health facilities.
According to statistics, about 10-15% of the couples in Uganda cannot have children due to infertility.
Nb
10 of such hospitals would never make the Country of Uganda broke but the army of 100,000 well armed African soldiers would.
In Uganda, The National Health Service Doctors, who have been on Strike for three weeks, have temporary suspended it until 16 December, 2017
A helpless young African patient lays on one of the hospital beds that have no medical doctors for the last 3 weeks.
24 November, 2017
By the Monitor newspaper, Uganda
UGANDA, KAMPALA- Patients can finally breathe a sigh of relief as normal health care service delivery in public health facilities are expected to resume effective Sunday, thanks to doctors’ decision to suspend their strike.
The doctors under the Uganda Medical Association (UMA), on Saturday voted to suspend their strike up to December 16, the date when the government promised to have delivered on some of their demands.
A Salary Review Commission is also expected to have come up with a resolution on the salary and allowance demands of the doctors, by that date.
The strike which started on November 6, has seen services in government aided hospitals paralysed with doctors listing a raft of demand s, including enhanced duty facilitation allowances, disbandment of the State House Health Monitoring Unit and a steady supply of sundries and other medical supplies in hospitals before they return to work.
Dr Ekwaro Obuku the UMA President, however, warned government not to take the doctors’ demands for granted since they would ill not hesitate to resume the strike if by December 16, if nothing tangible has come up.
“Doctors are eager to resume their Industrial action if not taken serious …and then [December 16] people [doctors] will be going for Christmas. We don’t know when they will return,” Dr Obuku warned amidst cheers from the medical workers who jam-packed Silver Springs Hotel’s Hall in Kampala.
The decision made at the end of their General Assembly on Saturday followed back- to -back meetings between the UMA’s national executive committee and Cabinet to end the industrial action.
State Finance Minister David Bahati who attended the doctors’ assembly pleaded with the doctors to resume work, admitting that government “had indeed been brought to its knees.”
“[Dr] Obuku has said you have brought us [government] to our knees. Friends, I am on my knees to ask you to consider these issues,” Mr Bahati said.
Mr Bahati reiterated the government pledges to the doctors including the supplementary budget for drugs and sundries, welfare and training of Senior House officers and intern doctors as well as duty facilitation allowances for all doctors in public service.
He said that during the current financial year, they have added Shs41 billion supplementary to National Medical Stores (NMS) to provide for emergency medical supplies.
He said the Ministry of Finance has been allocating Shs230 billion to NMS for the supplies and another Shs7.2 billion to Joint Medical Stores for the bureaus.
The minister said another Shs4.2 billion has been released to the Ministry of Finance to cater for the allowances of the Senior House Officers (post graduate doctors) , and the verification process is on-going to ensure the salaries go to the rightful people.
The interns will also have their allowances enhanced to Shs940, 000 from Shs740, 000 and be paid in every month as opposed to quarterly.
The enhancements are to act as a temporary measure to end the industrial action as the two parties proceed with the negotiations.
Out of the 295 doctors who attended the assembly, 113 voted to suspend the strike while 76 voted to continue with the strike while the rest abstained.
None of the doctors voted to call off the strike indefinitely.
lnamagembe@ug.nationmedia.com
In Uganda there is an Impasse: The government has come out and spoken the truth of the matter to the medical staff on strike:
November 15, 2017
Written by URN
Government has maintained its stand that it cannot negotiate with Uganda Medical Association (UMA) on the welfare of medical workers.
Minister of Health, Jane Ruth Aceng reiterated the government's stand in a meeting with the striking medical workers at Statistics House today morning.
Aceng noted that UMA isn't a trade union and therefore can't negotiate with government on the medical worker's welfare. She explained that the ministry appreciates the working conditions of the medical workers, saying they are committed to improving the situation.
The meeting yielded no results
Attorney General, William Byaruhanga also told the leadership of UMA that the mandate to negotiate with government lies with trade unions as provided for in the 2008 Labour Union Act.
"We have just come here to address you, we can talk to you as an association but we cannot negotiate with you. You should know that. This is information that you need to know" Byaruhanga said.
Adding that, "Government will adopt plan B if you fail to return to work. Our priority is the patients who have not been attended to. We request you to return to work."
However, this infuriated the doctors, escalating the already tense mood in the room. The doctors told the six cabinet ministers present including David Bahati (state minister for planning), John Chrysostom Muyingo (minister of state for higher education), Mwesigwa Rukutana (deputy Attorney General) that without addressing their concerns and issuing more threats of moving to "plan B" they had simply wasted their time.
UMA president Dr Ekwaro Obuku said if government is ready to move to "plan B" the doctors are determined and ready to move to "plan C". Obuku said government was "being unserious" about the entire situation and was not caring about the patients who are losing lives because of lack of medical care.
Minister Bahati had called on the doctors to be patient with government for at least another two weeks and call off the strike as they they institute a salary review commission to harmonise all civil servants' salaries. It is over a month since the prosecutors laid down their tools in protest against poor pay.
The doctors however demanded written commitment from government, saying they always make promises that they don't keep. Workers MP Sam Lyomoki said he had never before met six "powerless" ministers who wasted time doctors' time by calling for a dialogue yet they had no solution.
Bahati said government can't commit itself on a recurrent expenditure without first identifying the source of the money. Deputy Attorney General, Mwesigwa Rukutana told the striking intern doctors that they can't call themselves doctors and can't demand salaries. He explained that what interns are paid is an appreciation, which can't be termed as an allowance.
Rukutana asked the intern doctors to drop their demands and return to work. Doctors laid down their tools on Monday last week following protracted negotiations with government to give them a pay rise and improve their welfare in vain.
They vowed not to resume work until government addresses their concerns. The doctors want government to increase the salary of medical interns from Shs 960,000 to Shs 8.5 million.
They also medical and teaching assistants to earn Shs 15 million, get a two-bedroom house and a 2.5cc vehicle. They also want government to pay a senior consultant doctor or professor Shs 48 million including allowances; provide him a five-bedroom house, 4.0cc vehicle and three domestic workers.
Currently, a senior consultant doctor earns about Shs 3.4 million, consultant Shs 2.6 million, and a medical officer Shs 1.1 million. The doctors also want salaries for nurses and midwives enhanced to about Shs 6.5 million besides providing them a three-bedroomed house, 2.0cc vehicle and one domestic worker.
Nb
So if these doctors are given a house to live in without paying rent, and then given domestic workers, will they allow their workers to join the UNION? Most countries really do not have such luxuries for their medical staff and they really work hard and love their jobs.
In Uganda, All the medical staff that have gone on strike because of very low wages, have been given an order to return to work:
Health minister Jane Aceng. FILE PHOTO
09 November, 2017
By EMMANUEL AINEBYOONA & ABUBAKER LUBOWA
UGANDA, KAMPALA. Health Minister Jane Ruth Aceng says Uganda Medical Association (UMA) that organised the strike is not a registered union to lobby for labour rights.
She orders all doctors and intern doctors to resume work at once; directs UMA officials to stop interfering with Association members willing to work; promised protection for doctors who get back to work; and, says intern doctors who fail to comply will have their internships terminated and have to reapply.
Health workers who were misled but realise their mistake and resume work will not be subjected to disciplinary procedure, she says. In An 8-point terse statement read at a press conference on Thursday night at Health ministry headquarters in Kampala, Dr Aceng says the doctors never gave formal 90-day notice and followed no public service procedure in declaring industrial action.
She says grievances about salary and working condition by public officials must have been channelled through the Public Service Negotiation and Consultation Council. This, she says, is the guidance by the Solicitor General, the technical arm of the Attorney General, the government chief legal advisor.
Dr Aceng tells the ongoing press conference that they, however, appreciate the doctors’ concerns as “genuine”. She says the Office of the President directs all Resident District Commissioners (RDCs), who represent the President in districts, to monitor compliance of doctors with the new directive.
eainebyoona@ug.nationmedia.com
Nb
Are these Uganda medical staff kids, that have been misled badly, by some mature bad medical staff?
Wano e Buganda amalwaliro gonna agaddukanyizibwa governmenti ya Uganda tegakola, kubanga abasawo beddimye okukola, olwokufuna omusala ogutasobola kubabezawo:
Akulembera emivuyo gino gyonna wano Ebuganda akwate abasawo bano abaggalire e Luzira nga bweyalabudde. Kubanga abalwadde bajja kufa okusinga nga bwebabadde!
In Uganda, the Ministry of Health is unable to run its Hospitals because the Medical University of Makerere was closed by President Museveni and his wife:
FRIDAY NOVEMBER 11 2016
Makerere University medical students at the College of Health Sciences discuss during a meeting in a move to reject a call for them to resume working in their respective hospitals of deployment before the university is open .
PHOTO BY COLLEB MUGUME
By LILIAN NAMAGEMBE
UGANDA, KAMPALA:
Ministry of Health has said there is nothing they can do to solve the medical personnel shortage at Mulago Hospital, subsequent to the withdrawal of over 300 postgraduate medical students who also treat patients as part of their medical studies. Mulago Hospital and the subordinate city division hospitals of Kawempe and Kiruddu and other Kampala Capital City Authority health centres said they were strained by the high turnout of patients following the president’s directive to close Makerere University last week.
Dr Asuman Lukwago, the outgoing ministry of health permanent secretary, said the education ministry was responsible for the university and therefore, there is nothing his ministry could do to save the situation. “We would be contradicting ourselves. Ministry of education is responsible and not us as ministry of health. There is nothing we can do,” Dr Lukwago told daily Monitor in a phone interview. However, an earlier directive by the education minister, Ms Janet Kataha Museveni, to open the College of Health sciences to enable the students and lecturers to resume their studies was also defied by the latter.
The postgraduate students did not budge, arguing that government was subjecting them to “modern day slavery” since they are not paid to treat patients. Several meeting between the postgraduate medical students and the administrators at the college of Health science to convince them to go back to the hospitals did not bear fruits. “We have unanimously decided to maintain our stand not to go back to the hospitals until the University is open and our lecturers have reported on duty,” Dr Solomon Kyazze the president of the post graduate medical students’ association told Daily Monitor after a closed door meeting. Dr Alexander Bangirana, the Assistant Clinical Head accident and emergency, said the causality ward in Mulago Hospital which receives over 100 patients on a daily basis is strained by the personnel crisis.
“The initial health care is available but there is a shortage of specialists,” Dr Bangirana said. To improvise the available staff, Mulago hospital spokesperson, Enock Kusasira said the hospital has resorted to giving more attention to critical cases considered as life threatening. “We are concentrating less on out patients especially those whose cases are not life threatening,”Kusasira said. At the hospital, patients have to wait for hours before seeing the health workers. The case is not different from other affiliate hospitals and health facilities.
On a daily basis, Mulago handles over 10,000 patients, 4,000 of whom are in-patients.
lnamagembe@ug.nationmedia.com
The Supreme Court of Uganda has ordered its Constitutional Court to listen again to the case of why many pregnant women are dying in Uganda:
Written by URN
Last Updated: 30 October 2015
Mothers undergoing postnatal care at Mulago Hospital
Seven Supreme Court judges have unanimously agreed and ordered the Constitutional Court, to hear a case lodged against government in 2011, over its failure to provide basic maternal health kits for expectant mothers.
The decision of the highest court strikes down the earlier ruling of the Constitutional Court, in which, it dismissed a case regarding the alleged violation of health rights of women and mistreatment of expectant mothers by health officials.
The Constitutional Court, in 2012 dismissed the case on the advise of the Attorney General that the petition was of 'political nature' that necessitated allocation of more funds to the health sector by the executive - something which court couldn't determine.
Today, justices; Esther Kisaakye, John Wilson Tsekooko, Galdino Okello, Jotham Tumwesigye, Benjamin Odoki, Christine Kitumba and Chief Justice, Bart Katureebe faulted the lower court for having erred in law, when they declined to hear the case.
Core to the petition is that government's refusal to provide essential maternal health services for pregnant women is a violation of their right to life and good health.
The case was lodged by a civil society group, Centre for Human Rights and Development (CEHURD), and two families who appealed against the earlier Constitutional Court ruling in the Supreme Court.
The petition cites two examples, whereby Sylvia Nalubowa (daughter of Rhoda Kukiriza) died from Mityana hospital due non-availability of maternal health kits in a government hospital. Also cited is Anguko Jennifer (wife to Inziku Valente) who is said to have died while giving birth, on allegations that the nurses adamantly refused to attend to her.
“I would therefore find that although the political question doctrine has limited application in Uganda, the Constitutional Court erred in law when it struck out the appellant's petition without hearing it on its merits on grounds that they had no jurisdiction and that the petition raised political questions…,” ruled Kisaakye.
“In conclusion, I would allow the appeal and make an order directing the Constitutional Court to proceed and hear the constitutional petition No. 16 of 2011 on its merits,” added Kisaakye.
Court ordered each party to bear its own costs on grounds that it was not the fault of either party that the petition by civil society was not heard on its merits.
In a press statement, CEHURD welcomed the ruling and praised the judiciary for standing up with the rights of the women.
An American lady, Mrs Melinda Gates is urging health institutions to achieve their human health goals as they work to save lives:
Written by Shifa Mwesigye
Last Updated: 21 October 2015
Melinda Gates
The world will have to prioritise the health and wellbeing of women and children if it is to meet Sustainable Development Goals, the co-chair of The Bill and Melinda Gates Foundation has advised.
Speaking at the Global Maternal and Newborn Health Conference (Global MNHC) in Mexico recently, Ms Melinda Gates, from the Bill and Melinda Gates Foundation, said that newborns had been the forgotten community of the development agenda.
“For all the headway we have made on so many fronts, the hard truth is that progress on newborn health has lagged behind,” Ms Gates said.
The Global MNHC offers the first opportunity for policymakers, researchers, advocates, health experts and communities from over 75 countries to discuss evidence-based actions needed to achieve Sustainable Development Goals. It also targets development of a global strategy for women’s, children’s and adolescents’ health and reduction of maternal and newborn deaths.
The Bill and Melinda Gates Foundation invests $130 million annually in maternal and newborn health. Mexico, the host country for the conference, is credited for pioneering successful policies and programmes to improve maternal and newborn health. Globally, the fertility rate has come down to 2.5 children per woman, while nine out of ten girls attend primary school and life expectancy has increased to 71.
Ms Gates noted that the health of newborns was intertwined with the wellbeing of their mothers and the two could not be separated. In particular, Uganda’s maternal mortality ratio has decreased from 780 deaths per100,000 live births to 360 deaths per 100,000 live births, although Uganda did not reach MDG 5 of 200 deaths per 100,000 live births, according to the Gates Foundation statistics.
Under-five mortality rate decreased from 187 deaths per 1,000 live births to 55 deaths per 1,000 live births, reaching MDG 4 target of 62 deaths per 1,000 live births. However, this is not enough.
The aim of SGD 3 is to reduce newborn mortality to at least 12 per 1,000 live births, under-five mortality to at least 25 per 1,000 live births; and maternal mortality to less than 70 per 100,000 live births by 2030.
PLAYED PART
The Bill and Melinda Gates Foundation has invested in building maternal homes across Africa so that as their due date nears, women are accommodated here. This eliminates the first delay that often puts millions of women’s lives in danger, the delay to reach a health centre.
While at maternal homes, pregnant mothers can learn about the benefits of eating well, breastfeeding, family planning, personal hygiene, and immunization.
The foundation also rallies governments around the world to increase their budgets to family planning. At the 2012 London conference on family planning, President Yoweri Museveni pledged to provide $5 million every year for five years for buying contraceptives and providing them to women who need them. Ms Gates says research has proved that helping a woman plan and space her pregnancies is the most effective way to save mothers and newborns.
EMPOWERING GIRLS
“It doesn’t end there. If women space their pregnancies, they are more likely to have healthy babies. If their babies are healthy, they are more likely to flourish as children.When health improves, life improves by every measure. Better health leads to better education, which leads to better economic opportunities, which lead to broader prosperity for communities and countries,” she said.
A mobile phone-based national health survey in Uganda, supported by the Bill and Melinda Gates Foundation, revealed that young people weren’t using family planning services. With this evidence, government is now prioritising young people in Uganda’s national family planning strategy.
Dr Babatunde Osotimehin, the executive director of the United Nations Population Fund, noted that the discussions and decision made about adolescent girl will help in achieving SDGs because she is the entry point to the success the world is going to have. He argued that a girl who goes to school and stays there doesn’t get pregnant, especially if she uses contraception.
He warned that the ability of a woman to decide what to do with her body should not be the decision of any man.
“Why should he tell her when to or when not to have children?” Osotimehin said. “Why should we, in 2015, be dealing with the maternal mortality? If we can empower women to make their own decisions, we will achieve a lot in human development. The 225 million women in the world who want FP [family planning] must now get it,” Osotimehin said.
"Tearful to see fellow women suffering in poor medical health treatment or care;" Melinda Gates really feels it and says it:
Written by Shifa Mwesigye
Last Updated: 22 October 2015
Melinda Gates
When Melinda Gates and her husband Bill went on safari to Zaire, they wanted to see animals. But they quickly realized that the world they were visiting was different from the world they were accustomed to back home in the United States, people were burdened by disease, poverty and lack of information.
Shifa Mwesigye spoke with Melinda Gates, the co-chair of the Bill and Melinda Gates Foundation on the sidelines of the Global Maternal Newborn Health Conference in Mexico City about what her foundation has done to tune these misfortunes around in developing countries.
The conference came a month after the ratification of a new global framework for sustainable development, with ambitious new target called the Sustainable Development Goals.
Way back when the foundation was formed, what was the case, the voice or the story that made you start walking this walk and start this foundation?
When Bill and I got engaged, neither of us had ever been to Africa. That was in 1993. We took our first trip to Africa to go to this park in Zaire and see the animals. I loved the animals and I still love going to safari but we were really really touched by the people.
It really started a series of questions for us. This was just a few months before we go married. We had committed that we were going to take a beach vacation and we were going to talk about what we were going to do with the resources from Microsoft.
At the end of this trip, we decided that the vast majority of the resources that come from Microsoft were going to go back to society. When we were in Africa, these questions kept coming. Why was it that when we drove down the road, we would see towns shut down, open air markets, not great roads, men with flip-flops and smoking quite often?
A woman with a baby in the belly and one on the back and often with a huge bundle of sticks on her head that she was taking to the market. We couldn’t get what was going on. Why would we fly from the States to Nairobi and have kind of a similar experience but then you get out in the rural areas, completely different.
Six months later, we read that one of the biggest killers in the world was diarrhoea. We were like, diarrhoea? Kids don’t die of diarrhoea. In the United States you go to the drug store, get a drug and if it is really bad you go to the doctor. And we started to learn that there was this huge lag that when a vaccine came out of the United States or UK or Japan, it took 20 to 25 years before it got to Kenya or Tanzania or Uganda.
We said, that doesn’t make sense and it seems that there are so many broken things that can be fixed. So we started to learn about what a foundation could do to fix them. And that really ignited our passion. There is a huge inequity in this world, we all have equal lives whether you are born in Nairobi or New Delhi or Johannesburg - all lives have equal value. But it’s clear the world doesn’t treat them that way. So we would take the vast majority of resources from Microsoft and try to bring up the health equity. That is kind of how we got started.
What drove you to start working with women and girls and to address reproductive, maternal and child health challenges?
I have been really fortunate, for the last 15 years, to travel on behalf of the foundation. I am out in the developing world about three times a year. I would be out talking to men and women and when the men would go back to the fields, I would stay out talking to the women about their children and vaccines. The women would bring the conversation back around to reproductive health.
Particularly in African countries, they would ask ‘what about that shot I used to get in my arm. I walked ten kilometres to the clinic and I would get it. Now I go there for immunisation but it is stocked out, I don’t know what to do’.
I ran into so many women who were outraged that they couldn’t have access when they wanted. They would say ‘I have five children, I can’t feed another one much less put them in school’. As I would come home, I started to sift through the data about contraceptives. I realised condoms were stocked around the world because of the various AIDS programs. But women would tell me they couldn’t negotiate a condom with their husband because if they did, it would suggest that she has Aids or he has Aids.
So I started to look at the huge need of 210 million women asking for contraception and I just said we had to do something about it. And that is why in 2012, we met partners at the London Summit on Family Planning and we raise $2.3 billion with a goal to give voluntary access for family planning to 120 million women. Once we committed that to the world, low, middle and high income countries started to come forward and said ‘I will come up with a country plan on what I want to do for my country’.
The great news is the African countries are coming up with their own cost effective family planning plans and the donor community can decide how much of those plans they can fund and if it is missing funding, they will go out and try to get a private donor. So my passion has come from the voices I have heard of so many saying they want this and they need it. It’s a life and death crisis for them and their families.
Your foundation has done a lot of work in terms of access to contraceptives. I want you to address the myths and misconceptions that continue to prevent women from accessing contraceptives.
The misconception I have heard the most is that contraceptive tools cause sterility which is just completely false. Yes, we should all be concerned about our health and anything we put in our body. You have to make sure that whatever tool you put out goes through the very best regulatory body and authority.
In USA there was a misconception for over 20 years that there was a certain vaccine that caused autism in children. It meant that families were backing away from it. As you know when a myth starts it gains momentum in communities. The same was true particularly in northern Nigeria where they thought that this is a western plot to introduce sterilisation.
That has spread to other African countries as well. Now we going and really telling people the truth. We are using local community workers to say that these are the facts, ‘I use it, my aunt uses it, my sister uses it and I still have more children because I haven’t been sterile’. Getting other women to talk about the reality and their person experience, that is how you burst through the myths.
In Sub-Saharan Africa, you have been there and many countries are still struggling with maternal deaths. What can be done to reduce such cases?
The great thing is that in countries like Malawi, they realised that the biggest problem was out in the villages. Even though the public policy was put out, they started to realise the implementation of the policy wasn’t working. They had to get women to come into the clinic and come in early.
So now they are building maternity waiting homes so that they have a place for women to wait when they come to the clinic. They have transport to pick them up a month ahead. They are also training midwives out in the villages so that you will have incredibly well trained midwives. Having a train skilled birth attendant in the communities, we are starting to see some downward trend on maternal mortality rates.
The last thing is bringing the tribal chiefs along in the plan. You have to get the men and boys involved when you talk about women and girls because they are often the ones making the decisions and providing them resources.
15 years later and over $30 billion investment, what have been your achievements particularly in Uganda? What lessons have you learnt from your work and how do you feel when you launch a program in a country, invest in it and when you leave it closes?
Of course not very good. Your question hits the nail on the head. If we go and do work in any country and the country doesn’t see it as their work and they don’t own it, it is not going to be sustained.
Everything that our foundation does, we try to do it in partnership with governments. That is not always easy, sometimes it slows things down, but the government has to own it because if they own it they will maintain it and they will keep adding to it - same thing about local communities.
If you want to reach a girl or woman in a local community, you have to know where she is coming from. You have to understand the power structures that exist around her, what is holding her back and where the opportunities are to invest in her and give her a voice in decision making.
If you could get the local support to do some of these grassroots efforts, that is when you make progress. So in Uganda, we work with several of the youth groups to bring to light the issues going on in Uganda through plays and dramas.
We are also trying to highlight family planning in Uganda. The government finally made a commitment. It is small in terms of dollar commitment but they actually have a goal now for themselves. The fact that we have this resource at a global level that they can come for, we will start to see Uganda making some strides
What is your take on empowering communities and citizens to demand for safe motherhood?
I am a huge believer in empowering communities. All over the world one of the things we see is that if you have collective individuals who are not being given their rights, when they come together as a collective and approach the government, they are far more likely to make progress.
We saw it in India with HIV and Aids were men and women who had HIV and Aids demanded for their rights, saying ‘I have a right to the medicine and you cannot discriminate against me’. Then the government started giving out the services. So in Africa we are seeing citizen groups demanding for services, it pushes the governments to do the right thing and it pulls the services through. The only way you can achieve this citizen advocacy is that they have to be home-grown, they have to be generic.
Trainers have to come from the communities because then people listen to them and this makes much more sense.
Melinda Gates visits a newborn at Wakhinane health post in Dakar Senegal. Photo: Frederic Courbet
As you have seen travelling around Africa, problems for African women are many, does this burden you or it drives you more?
I see huge problems in Africa from female genital cutting to child marriage but is the world as a whole getting better for women? Yes, and I see it particularly in the urban places that I go to [like] Arusha in Tanzania or Nairobi. Still you have places where you have slums on the edge but we start to get changes.
The way we know that life is improving is, by measuring things like income, poverty reduction, maternal mortality and childhood mortality. A woman bears the extra burden or responsibility if her child is sick compared to the man. The fact that malaria deaths are down by 40% means that things are better not just for the people who had the malaria deaths but for the woman in the household. I certainly carry it heavily when I am in Africa or Bangladesh and it is tearful.
I go back to the hotel and weep because I have seen some very horrific things happening to women. I see hope and I see progress. When I see a woman in Bangladesh or Kenya and she is starting to make money payments over her phone, when she can get a remittance on her phone and she has access to her own finances, wow, that is progress.
I am starting to see these innovations taking hold and what I want to see is that they take hold equally. Women are still behind by 21% in cell phone services. In banking services they are behind by 40% but the great thing we can do is to stimulate the cell phone companies to market and get the services to women. So I think there is a lot of progress for women and those are the things that I hang onto and they keep me hopeful on some of the dark things.
You mentioned earlier the challenges in USA on maternal death, why is that so in a developed country like USA and what can Ugandans and Rwandans learn from the American challenge?
One of the mistakes the United States made is that we got to a certain point and we didn’t keep investing. Certain areas in the rural US, in the south and some of the big urban area like [Washington] DC have terrible maternal mortality rates [and] in the places where we have the most impoverished people - we haven’t continued to make the investment.
In the places where we have the most impoverished people, we haven’t continued to make the investment. That needs to happen because we know what to do but we just aren’t doing it as a country. We try to get the government to go back and reach the women with the right messages around contraceptives.
These outreach health models in African where the local community adds up to the next clinic that eventually adds up to the tertiary hospital, United States needs to invest more in these community health workers that go out and give mothers prenatal and post natal visits, immunisation and family planning.
We understand that malaria and HIV are difficult viruses and diseases to solve. But why are 2.5 billion people around the world are still living without toilets? Is there a lack of political will regarding this? And lives are being saved but they are not being transformed, is this failure of global policymakers?
It is not just about surviving, it is about thriving. What I like about the new SDGs is that we are saying it is not enough to make sure a child lives. How do you make sure they thrive? If they are born healthy and they get the right vaccine, they live to age five. If you don’t make the right nutrition investment, that child is not going to grow up to reach their full potential.
They are not going to be able to learn in school, they will not participate in the economy the right way. So we have to look at all the health investment, education investment. So it is not enough to grow up healthy, you have to make sure you are educated properly and that you can participate in society. To me sanitation is just one of those basics that everybody should have a right to.
One of the things the foundation is investing in is a waterless toilet. We can build a more efficient toilet that doesn’t require water. The output from it can be used and recycled back into the land as fertilizer. So we have deep investment trying to reinvent the toilet and it will help with diarrhoea but also help with dignity.
Why then is such an obvious thing taking so long for the world to understand? Why the lack of political will because sanitation is such an obvious thing. It affects everything all kinds of health policies.
You could ask yourself the same about vaccines 15 years ago. Vaccines are one of the lowest cost innovations but it’s about how do you make investment as a government for your people. Whatever reasons the governments hasn’t made investment in sanitation, they ought to do it.
The National Medical Stores (NMS) has dismissed claims that there is a shortage of drugs and sundries in the country of Uganda.
The Government Medical Stores at Entebbe are all full up with medical prescription drugs to service over 2500 outlets for the public health clinics and hospitals.
“I get disturbed when I hear anybody saying there they do not have Mama Kits or even ARVs for instance.We do not have any shortage. In fact what we do not have is enough space for all the batches. As I speak we have our containers at Nakawa. We only get space when we receive more orders,” said the NMS executive director, Moses Kamabare during a media tour of the drugs warehouse at Entebbe yesterday.
Kamabare said NMS delivers medicines, sundries and laboratory supplies to all the 2900 public health facilities across the country.
“For all government and accredited facilities, we supply them twice a month according to orders.For regional referral hospitals, we do deliveries once every month,” said Kamabare.
“We have a system that enables us to process emergency orders within 24 hours. We also work on weekends and public holidays, but some hospitals often let us down. They may tell you they are not open on weekends, yet the patients are stuck,” he added.
%uFFFC
All the modern drugs are available even if one finds lots of this type of medical stocks in the normal private chemist shops in the city of Kampala. They are sold at very high prices.
He further explained that some of the health facilities were not affiliated to the drug delivery system.
“If there is a new facility in your village, it misses out unless it receives certification from the health and finance ministries,” said Kamabare.
This website would like to store cookies in your web browser to help improve the site. About cookies.Allow Cookies








 A source, also a doctor at the facility told authorities that the mother came to the hospital for checkups after her pregnancy started showing complications but was later discharged by one Dr. Thomas Data who is also an intern.
A source, also a doctor at the facility told authorities that the mother came to the hospital for checkups after her pregnancy started showing complications but was later discharged by one Dr. Thomas Data who is also an intern.

 The mortuary at Mulago Hospital. File Photo
The mortuary at Mulago Hospital. File Photo



 Contraceptive use said to be higher in marrieds than the single
Contraceptive use said to be higher in marrieds than the single



 Mulago Hospital’s Enock Kusaasira touring the new specialised maternal and neonatal center. Photo by Mary Kansiime
Mulago Hospital’s Enock Kusaasira touring the new specialised maternal and neonatal center. Photo by Mary Kansiime Arabs Contractors’ Tarek Eldakdoky (left) giving t Kusaasira a tour of the center. Photo by Mary Kansiime
Arabs Contractors’ Tarek Eldakdoky (left) giving t Kusaasira a tour of the center. Photo by Mary Kansiime